Simple Airway Adjuncts
Two simple airway adjuncts are commonly available:
Nasopharyngeal airway
This device is designed to be inserted via the nostril into the back of the mouth, with the aim of creating a patent passage behind the tongue. Traditional teaching about sizing this device included choosing a size similar to that of the patient’s little finger, and similar in length to the distance from the tragus to the tip of the nose. These teachings have fallen out of favour and now the device should be compared with the patient’s nostril internal diameter to find an appropriate size.
The device should be inspected to ensure it is patent. It should have a large flange to prevent aspiration. If there is not a large enough flange, then a safety pin should be inserted through the end of the airway. Care should be taken to ensure that a suction catheter could still be passed down the lumen of the device. Lubrication (with a water-based gel) should be applied to the outside of the device. If this is not available, then use the player’s own saliva.
Many rugby players will have previously sustained nasal trauma and therefore the nose should be inspected to determine which nostril is most likely to allow passage of this airway.
The nasopharyngeal airway is then inserted along the floor of the nose (i.e. at approximately 90 degrees to the face) – note it should not be inserted “up” the nose. Mild resistance may be felt – this is likely to be the nasal turbinates and is easily overcome by gently rotating the airway. Once inserted, the airway should be reassessed. Care should be taken when inserting this device as it can cause epistaxis, which can worsen the airway problem.

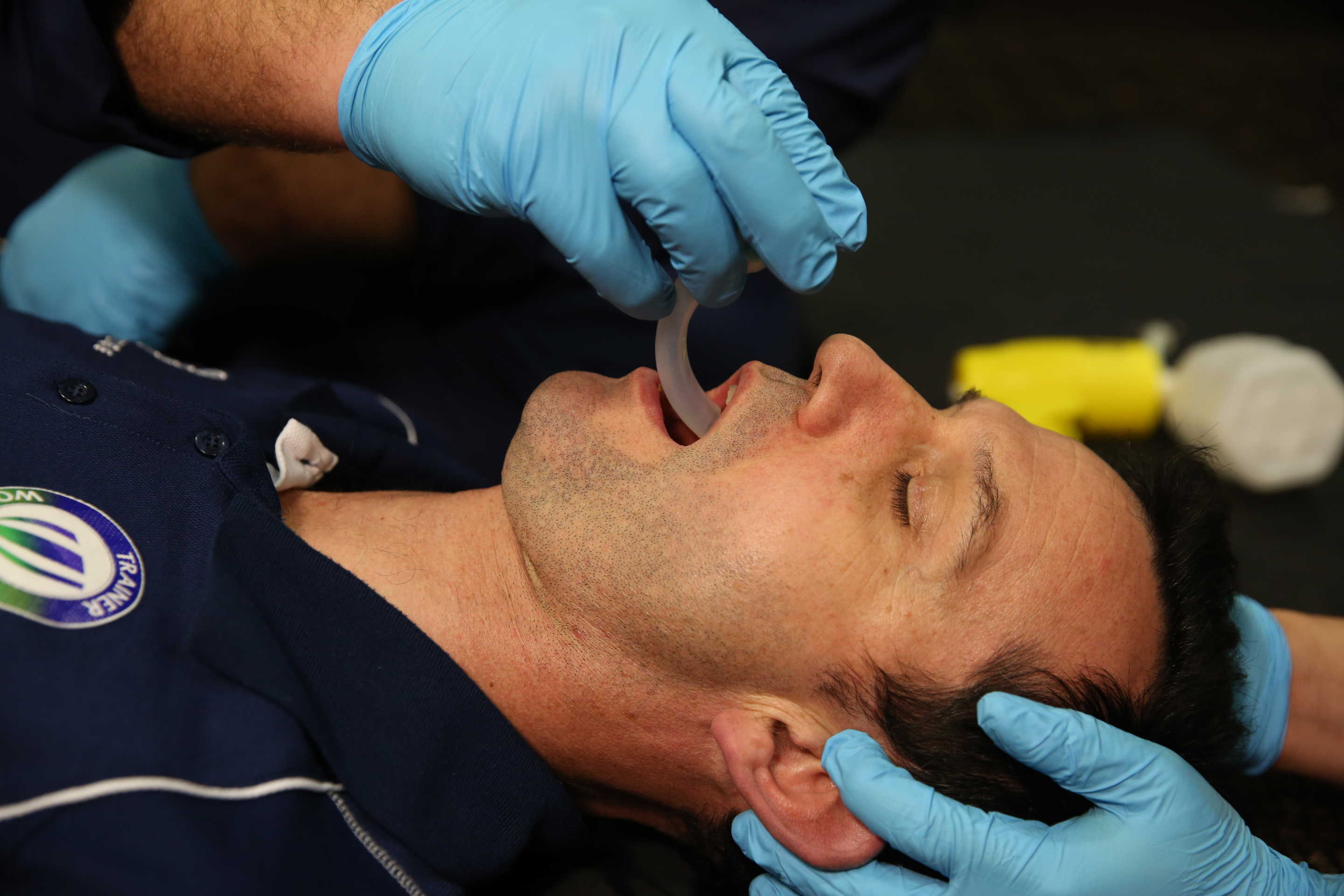
Insertion of a nasopharyngeal airway
Oropharyngeal airway (OPA)
The oropharyngeal airway is designed to be inserted via the mouth, with the rigid plastic passing beyond the tongue, lifting it forward, creating a patent airway.
There are several ways to size an oropharyngeal airway. These techniques are all acceptable and all achieve the same endpoint, which is to choose a device that is long enough to successfully create a passage behind the tongue, without being so long that it causes laryngospasm.

Sizing of OPA: incisors to the angle of the mandible
Previous teaching has been that in the adult population the device is carefully inserted “upside down” and then rotated through 180 degrees. Newer teaching is that the device is inserted under direct vision the “right way up”, using a tongue depressor or laryngoscope blade to lift the tongue forward. The device should be inserted with great care since it is easy to inadvertently cause trauma to the soft or hard palate. Once inserted, the airway must be reassessed.
OPA insertion inverted technique

OPA insertion direct technique with tongue depression
Naso or Oropharyngeal airway?
To tolerate an oropharyngeal airway, the player must be deeply unconscious. If this is not the case, there is a significant risk of the patient vomiting, compounding any airway problems. A nasopharyngeal airway is much better tolerated but may not be as successful at opening the airway. A decision must be reached in each case about which device should be used.
If a patient does not tolerate a jaw thrust, then it is most unlikely they will tolerate an oropharyngeal airway. In this case a nasopharyngal airway would be more appropriate.