Open Pneumothorax
This injury is a result of a penetrating injury which breaches the chest wall, resulting in a pneumothorax and a direct communication between the inside and outside of the thoracic cavity. It is also known as a “sucking” chest wound. If the hole in the chest wall is greater than two thirds of the diameter of the trachea, air is sucked into the thoracic cavity through the wound rather than through the trachea. This means that gas exchange in the alveoli will not occur.
On some occasions the communication via the chest wall remains patent, and the pneumothorax remains “simple”. However, sometimes the soft tissues act as a valve, which can lead to the pneumothorax “tensioning”. It is important that these patients are monitored closely, so that a tension pneumothorax can be promptly treated if it develops.
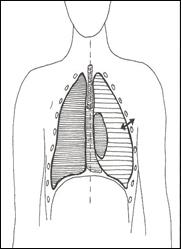
Pictorial representations of an open Pneumothorax
Recognition of an open pneumothorax
The defect in the chest wall is usually readily apparent if looked for. Examination for a pneumothorax and haemothorax should follow the standard approach.
Management of an open pneumothorax
- ABCDE approach
- High flow oxygen via non-rebreath mask
- Cover the defect
- This should be done by using a dressing which is sealed on three sides. This will act as a flap, which will allow air to move from the thoracic cavity outwards, but not into the thoracic cavity. This should prevent the pneumothorax from deteriorating to a tension pneumothorax.
- Commercial devices such as the Russell Chest Seals® are available to be applied over the wound. These seal have a valve(s) which will allow air to escape from the thoracic cavity, but will stop air moving in. They are lightweight and easy to apply
- Rapid Transfer to the Emergency Department

Russell Seal®