Surgical Airway
If all other techniques to obtain a patent airway fail, then the patient is likely to rapidly deteriorate and suffer a cardiac arrest due to hypoxia. Rapid intervention is therefore required. A surgical airway is potentially lifesaving in this situation. The two surgical airway techniques taught on this course are needle cricothyroidotomy and surgical cricothyroidotomy.
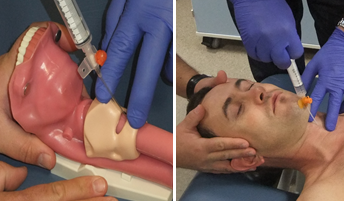
Needle Cricothyroidotomy
The needle cricothyroidotomy is a technique to insert a cannula through the cricothyroid membrane into the trachea. This membrane is located in the anterior neck, below the easily palpated thyroid cartilage and above the cricoid ring. A syringe should be attached to the back of a large bore cannula. This cannula is inserted through the cricothyroid membrane, at a 45 degree angle, pointing caudally (towards to patient’s feet). Once the tip of the cannula lies in the trachea, air can be freely aspirated into the syringe.
At this point the cannula should be advanced forward over the needle and the needle removed. The cannula then needs to be attached a high flow oxygen source to provide intermittent oxygenation. There are several techniques to achieve this, perhaps the most efficient way to do this is to attach a 3 way tap between the cannula with oxygen tubing attached to one of the other ports. This will leave one port open which should be used to provide intermittent oxygenation to the patient. This is achieved by occluding the spare port for 1 second and then opening it for 4 seconds. This is then repeated in a cyclical manner, so that oxygen is being driven into the patient for 1 second out of every 5.
Needle Cricothyroidotomy
This technique does not ventilate the patient, as it does not support gas exchange, it only allows oxygenation of the patient. For this reason, this technique is only a temporising measure and will allow up to approximately 20-30 minutes before a more definitive procedure should be undertaken. This window can be lifesaving, and the value of this procedure should not be underestimated.
There are numerous potential complications of this procedure and by understanding the local anatomy, the practitioner will be able to reduce and anticipate problems. Complications include; (but are not limited to) malposition of the cannula (with subsequent emphysema, haemorrhage or oesophageal perforation), hypoventilation, barotrauma or thyroid trauma.
Surgical Cricothyroidotomy
This technique involves a surgical incision through the cricothyroid membrane to allow passage of a definitive airway device. This is ideally with size 6.0 cuffed endotracheal tube in male players, with possibly a slightly small size cuffed tube for women.
Since this provides a larger bore than the cannula of a needle cricothyroidotomy, it supports ventilation, not simply oxygenation. However, since an incision is required, there is a greater risk of complications.